- Healthcare regulatory compliance covers more than HIPAA: the regulatory landscape includes HITECH, state privacy laws, billing and fraud statutes, and information blocking rules, and which ones apply depends entirely on your entity type
- A compliant posture is only as real as its evidence: access logs, audit trails, BAA records, and training attestations are what procurement teams and auditors actually verify, not policies alone
- Automation accelerates a working compliance program but does not replace one: organizations that skip foundational controls and go straight to tooling consistently find the same gaps, audit after audit
The deal is paused. Legal is asking about HIPAA. Engineering has flagged protected health information across three cloud environments. And nobody in the room can agree on what “compliant” actually means.
This is how regulatory compliance in healthcare usually becomes urgent, not through a planned program, but through a blocked contract, a stalled security questionnaire, or a sales promise that operations were not ready to back up.
The stakes are real and growing. In March 2026, the HHS Office for Civil Rights settled with MMG Fusion, a software business associate, after a breach that exposed the protected health information of 15 million individuals. The case reinforces a reality many organizations learn too late: compliance obligations extend well beyond the hospital walls.
This guide is an operational reference, not a legal glossary. Each section stands independently. The central argument is this: healthcare regulatory compliance in 2026 is a systems-and-evidence problem, not just a policy problem.
What healthcare regulatory compliance actually means
Healthcare regulatory compliance is the practice of meeting all applicable legal, regulatory, and contractual obligations that govern how an organization handles patient data, delivers care, manages billing, and operates its workforce. It is not synonymous with HIPAA, though HIPAA tends to dominate the conversation.
In practice, regulatory compliance in healthcare spans several interconnected dimensions:
- Data privacy and security
- Billing integrity and fraud prevention
- Patient rights and access
- Workforce conduct and training
- Vendor and third-party relationships
Each dimension carries its own obligations. Together, they form a regulatory environment that is layered, interconnected, and unforgiving of gaps.
The operational requirements are equally specific. A compliance program is only as real as its evidence, which typically includes:
- Access controls and role-based permissions
- Audit logs tracking who accessed PHI and when
- Encryption at rest and in transit
- Vendor oversight and documented agreements
- Incident response procedures
- Employee training records and attestations
What has made this harder in 2026 is the environment in which these requirements must be met:
- Cloud-first infrastructure has distributed PHI across multi-cloud environments, third-party APIs, and SaaS tools that organizations often adopt faster than they govern
- Artificial intelligence has introduced new exposure points, from clinical copilots processing patient notes to analytics platforms that may inadvertently use PHI for model training
- Healthcare clients have raised their expectations: an annual certification is no longer accepted as sufficient evidence of a controlled environment
Regulatory compliance in healthcare, then, is not a one-time audit outcome. It is a continuous operational state that demands ongoing systems, evidence, and accountability.
Who does healthcare compliance apply to?
Before mapping obligations, an organization needs to answer a more fundamental question: which regulatory category does it fall into? The answer determines everything from which rules apply to what evidence must exist.
Under HIPAA and HITECH, there are three distinct categories:
1. Covered entities
HIPAA covered entities include healthcare providers, health plans, and healthcare clearinghouses. They are directly subject to HIPAA’s Privacy Rule, Security Rule, Breach Notification Rule, and Enforcement Rule. This category includes:
- Hospitals and physician practices
- Health insurers and managed care organizations
- Pharmacies and healthcare clearinghouses
2. Business associates
Business associates are vendors, contractors, or service providers that process, store, or transmit protected health information on behalf of a covered entity. Key obligations include:
- Direct federal liability under HITECH, not just contractual exposure
- A signed Business Associate Agreement must be in place before any PHI is shared or handled
- Subcontractors of business associates carry the same obligations
Business associates carry direct federal liability under HITECH, as multiple OCR enforcement actions have demonstrated.
3. Neither category
HIPAA does not directly apply, but state laws may still create obligations. Texas Health and Safety Code Chapter 181, the Texas Medical Records Privacy Act, defines “covered entity” as any person who assembles, collects, analyzes, uses, stores, or transmits protected health information.
This is considerably broader than HIPAA’s definition and captures entities that fall entirely outside the federal framework.
Two questions help determine where an organization sits:
- Does your product or service touch protected health information?
- Does it do so on behalf of a healthcare organization?
If both answers are yes, the organization is a business associate regardless of how it describes itself.
The following table maps common company profiles to their likely compliance obligations:
When a hospital pauses procurement, it is typically doing one of three things: verifying BA status, checking whether a BAA has been signed, or requesting documented evidence that controls exist. This is not a bureaucratic formality. It is a legal verification.
For organizations navigating complex entity structures, BAA negotiations, or state law preemption questions, involving a healthcare regulatory compliance law firm early is a sound investment. Legal counsel is also essential if an OCR investigation is initiated.
The major regulatory compliance requirements in the healthcare industry
Understanding the regulatory compliance requirements in healthcare means recognizing that no single law governs the entire landscape. Several distinct frameworks apply, often simultaneously, depending on what an organization does and who it serves.
HIPAA: The operational baseline
HIPAA establishes the foundational rules for protecting electronic protected health information (PHI). HIPAA requirements fall into three categories:
- Administrative safeguards:
- Written policies and procedures
- Designated Privacy and Security Officers
- Workforce training programs
- Access management protocols
- Technical safeguards:
- Multi-factor authentication
- Encryption at rest and in transit
- Audit logging and activity monitoring
- Automatic session logoff
- Physical safeguards:
- Facility access controls
- Workstation and device security policies
- Media disposal procedures
When hospital procurement teams and auditors request documentation, they are typically asking for: access logs, security policies, incident response plans, signed BAA templates, and employee training records. HIPAA sets a compliance floor. State laws, contractual obligations, and sector-specific requirements can and do exceed it.
HITECH: The enforcement layer
The Health Information Technology for Economic and Clinical Health Act (HITECH) of 2009 did not replace HIPAA. It strengthened it considerably by making business associates directly liable under federal law, creating mandatory breach notification requirements, and introducing a four-tier civil penalty structure.
These provisions were formally codified into the existing HIPAA rules through the Omnibus Rule in 2013, which is why the Privacy Rule, Security Rule, and Breach Notification Rule, as they stand today, already incorporate HITECH’s requirements
Penalties are adjusted annually for inflation. As of January 28, 2026, Tier 4 violations, those constituting willful neglect with no corrective action, carry penalties between $73,011 and $2,190,294 per violation.
Since the Privacy Rule compliance date, OCR has settled or imposed penalties in 152 cases totaling over $144.8 million, with recent actions including a $1.5 million civil penalty against Warby Parker in December 2024 for Security Rule violations.
SOC 2, HIPAA, and HITRUST: What is the difference?
These three frameworks/standards are frequently confused. They are not interchangeable and do not substitute for one another.
A SOC 2 report does not make an organization HIPAA compliant. They address different problems: SOC 2 demonstrates security controls to enterprise buyers, while HIPAA compliance is a legal obligation governing how PHI is handled. Treating one as a substitute for the other is a common and costly mistake.
Beyond HIPAA: Other regulatory layers you cannot ignore
HIPAA and HITECH form the core of healthcare data compliance, but they do not define its edges. Depending on what an organization builds, who it bills, and where its data flows, three additional regulatory layers can apply with equal force.
1. Billing, fraud, and abuse: The financial compliance layer
Three federal statutes govern the financial side of healthcare regulatory compliance.
- The False Claims Act prohibits fraudulent billing to federal programs and carries significant whistleblower and qui tam exposure.
- The Anti-Kickback Statute restricts improper financial arrangements tied to healthcare referrals.
- The Stark Law governs physician self-referral arrangements.
These apply directly to platforms that touch billing workflows, referral management, or clinical decision support.
2. State privacy laws: The expanding layer
Federal law establishes minimum standards, but state legislatures have been moving considerably faster.
- Washington’s My Health My Data Act extends privacy protections to consumer health data well beyond HIPAA’s scope.
- For organizations handling data of EU residents, GDPR obligations around consent, data transfers, and patient rights apply in parallel.
3. Information blocking: The escalating enforcement priority
The 21st Century Cures Act prohibits practices that interfere with the access, exchange, or use of electronic health information. Enforcement penalties of up to $1 million per violation apply to health IT developers, health information networks, and health information exchanges.
In September 2025, HHS Secretary Kennedy directed HHS to significantly increase enforcement resources dedicated to information blocking, signaling an active and coordinated investigation posture going forward.
What healthcare organizations are actually expected to implement
The evidence that auditors and procurement teams ask for, covered in the above section, does not appear automatically. It is produced by the controls below. The five areas below reflect how procurement teams and auditors actually review vendors and healthcare organizations, and what evidence they expect to find.
1. Identity and access management
Access to protected health information should be granted on the basis of role, limited to what each role requires, and reviewed regularly. In practice, this means:
- Multi-factor authentication on all systems that access PHI
- Role-based access controls with documented permission structures
- Least-privilege enforcement, restricting access to only what is operationally necessary
- Periodic access reviews to verify that permissions remain appropriate
- Offboarding workflows that revoke access immediately upon departure
Evidence this produces: Access logs, provisioning records, and access review completion records.
2. Audit logging and monitoring
Logs are the evidentiary backbone of any compliance program. Systems that handle PHI should record who accessed the data, when, from where, and what changed. Retention periods vary by regulation and state law, but typically range from six years for HIPAA-related documentation.
The distinction that matters most during an audit is this: system-generated logs are verifiable and tamper-evident. Manual screenshots are neither. Organizations that rely on the latter consistently struggle to produce coherent audit trails under time pressure.
Evidence this produces: Timestamped access records, change logs, anomaly detection reports.
2. Vendor and third-party risk management
Every vendor that touches PHI is inside an organization’s compliance perimeter, regardless of how that vendor describes its own role. Cloud infrastructure providers, AI tools processing clinical data, analytics platforms, ticketing systems, and customer support tools all potentially handle protected health information. Each requires a signed Business Associate Agreement, documented security review, and ongoing oversight.
Evidence this produces: Subprocessor inventory, vendor risk assessments, and BAA tracking register.
3. Incident response and breach readiness
An incident response plan that exists only as a document is insufficient. Effective breach readiness includes documented escalation paths, breach notification timelines, designated response roles, communication templates, and regular tabletop exercises that test whether the plan actually functions.
Evidence this produces: Incident response plan, tabletop exercise records, breach notification templates.
4. Security awareness and workforce training
Most compliance failures do not originate in technology. They begin with an employee forwarding PHI to a personal email account, clicking a phishing link, or sharing credentials for convenience. Training programs should cover phishing resistance, safe PHI handling, remote work risks, and acceptable use of AI tools. Annual training is a minimum. Higher-risk roles typically warrant more frequent sessions.
Evidence this produces: Training completion records, policy acknowledgment attestations.
Where most organizations break down
- No documented asset inventory, so the PHI location is unknown or inconsistent
- Shared credentials across team members, making individual accountability impossible
- No formal access review process, leaving stale permissions in place for months
- Approvals and decisions recorded in Slack or email with no structured audit trail
- Missing or incomplete audit logs due to logging being disabled or misconfigured
- Policies documented and filed, but not operationally followed or enforced
- No evidence retention discipline, leaving organizations unable to demonstrate past compliance
The hardest part of healthcare regulatory compliance is usually evidence discipline, not policy creation. Most organizations can write a policy in an afternoon. Proving that the policy is actually followed continuously across every system and every team member is where compliance programs most often fall short.
Healthcare compliance in cloud environments
Cloud infrastructure has become the default operating environment for most healthcare technology. But choosing a cloud model does not resolve compliance questions. It relocates them.
Where data lives, who configures access, and how controls are enforced are decisions that belong to the organization deploying the environment, not the provider hosting it.
Public cloud, private cloud, and hybrid: What the choice actually means
For healthcare organizations asking which deployment model gives greater control over data and security, the answer is private cloud. A dedicated, on-premises or privately hosted environment gives an organization direct authority over infrastructure configuration, access controls, data residency, and audit mechanisms.
Public cloud environments, including AWS, Microsoft Azure, and Google Cloud Platform, offer considerable scalability and managed infrastructure under a shared responsibility model.
They are widely used for healthcare workloads and can be configured to meet HIPAA requirements. The compliance outcome depends entirely on how the environment is configured, not on which provider’s logo appears in the architecture diagram.
Hybrid approaches combine both, directing sensitive workloads to more controlled environments while using public infrastructure for less sensitive operations.
Common cloud compliance failures in healthcare
Most healthcare compliance failures in cloud environments do not originate in the provider's infrastructure. They originate in how organizations configure and manage the environments they deploy. Common patterns include:
- Overprivileged accounts with access far exceeding what roles require
- Unencrypted storage buckets or databases containing PHI
- Unmanaged or undocumented APIs creating unmonitored data pathways
- Shadow IT: services adopted without security review or visibility
- Missing or disabled audit logs, eliminating the evidentiary trail
- Poor vendor visibility into where PHI flows across integrations
Shared responsibility in AWS, Azure, and GCP
All three major cloud providers operate under an explicit shared responsibility model. The provider secures the underlying infrastructure, including physical facilities, hardware, networking, and the hypervisor layer.
Everything built on top of that infrastructure, including data classification, access management, operating system configuration, application security, and network controls, remains the customer’s responsibility.
This distinction matters because many organizations assume that a cloud provider’s compliance certifications extend to their own workloads. They do not.
A provider can hold a HIPAA-eligible service designation and still host a non-compliant deployment if the customer has misconfigured access controls, disabled logging, or left storage unencrypted. Saying “we use AWS” is not a compliance answer. Demonstrating how AWS is configured is.
How healthcare compliance audits actually work
Most organizations prepare for audits by gathering documentation. Experienced auditors do not start with documentation. They start with questions, and the answers either demonstrate a functioning compliance program or expose the distance between policy and practice.
What auditors actually focus on
The six areas below reflect what auditors and hospital procurement reviewers consistently probe, along with the specific question each area is designed to answer:
- Access control: Can terminated employees still access systems, or is offboarding reliably enforced?
- Audit trails: Can the organization prove, with system-generated records, who accessed PHI and precisely when?
- Vendor management: Do subprocessors and third-party integrations meet documented security standards, and is that verified rather than assumed?
- Endpoint security: Are employee devices encrypted, managed, and monitored, including personal devices used for work?
- Incident response: Can the team walk through an actual response workflow, or does the plan exist only as an unread document?
- Security training: Can individual employees demonstrate that they have received, read, and acknowledged current compliance policies?
Each question is designed to test whether controls are operational, not merely described.
Documentation-driven vs. System-driven compliance
How an organization has built its compliance program determines how well it survives this kind of scrutiny.
Why does evidence collection become chaotic
When audit preparation begins, most of the effort goes into locating evidence that should already be organized and accessible. Compliance responsibilities sit across multiple teams with no single owner. Systems do not communicate with each other, so evidence must be gathered manually from disconnected sources.
Log retention windows have lapsed, leaving gaps in the record. Approval decisions were made verbally or in informal channels, leaving no traceable documentation.
The audit chase is a symptom of a system’s problem, not a documentation problem. Organizations that treat compliance as a periodic exercise rather than a continuous operational state consistently face the same scramble, audit after audit.
A practical healthcare compliance roadmap for 2026
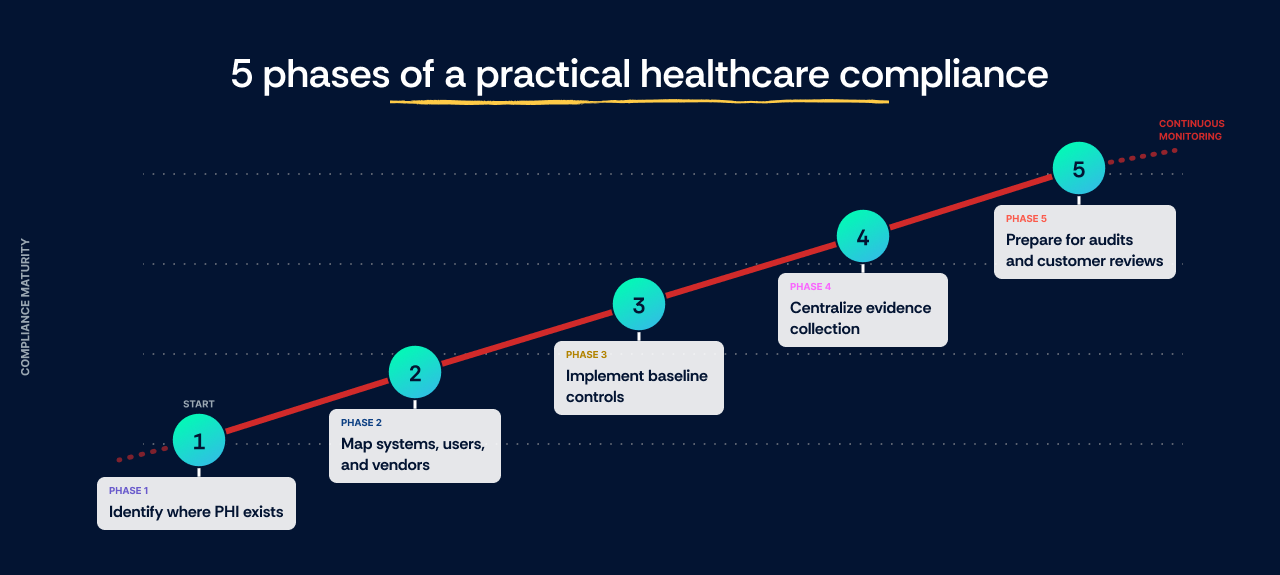
Compliance programs built under pressure tend to share the same flaw: they start with policies instead of starting with data. The five phases below are sequenced deliberately, each one creating the foundation that the next phase depends on.
Phase 1: Identify where PHI exists
Before any control can be implemented, an organization needs to know where protected health information actually lives. Cloud storage, support ticketing systems, AI tools processing clinical inputs, backup environments, and analytics platforms are all common locations. In most cases, PHI is present in more systems than the organization initially expects.
Phase 2: Map systems, users, and vendors
With PHI locations identified, the next step is mapping who interacts with that data. This means building a user access inventory, a subprocessor list, an integration map showing how systems share data, and an audit of any external sharing arrangements.
Phase 3: Implement baseline controls
This phase puts the foundational controls in place: MFA, encryption at rest and in transit, audit logging, backup testing, incident response planning, and workforce training. Controls documented in Section 4 of this guide apply directly here.
Phase 4: Centralize evidence collection
Controls without evidence are invisible to auditors and procurement reviewers. Logs, policies, approvals, access review records, and vendor agreements need to live in one accessible system, not distributed across spreadsheets, email threads, and shared drives.
Phase 5: Prepare for audits and customer reviews
With controls in place and evidence centralized, the organization should be able to respond to vendor questionnaires, procurement reviews, and formal audits without a panic-driven scramble. Continuous monitoring ensures the compliance posture remains demonstrable between audit cycles.
What these phases realistically require
The following table reflects typical effort levels for each activity, alongside what organizations achieve when compliance workflows are automated.
The highest hidden cost in this process is usually engineering time, not auditor fees. Every hour engineers spend pulling logs, documenting configurations, and chasing evidence across disconnected systems is an hour not spent on product.
What happens if a healthcare organization fails compliance?
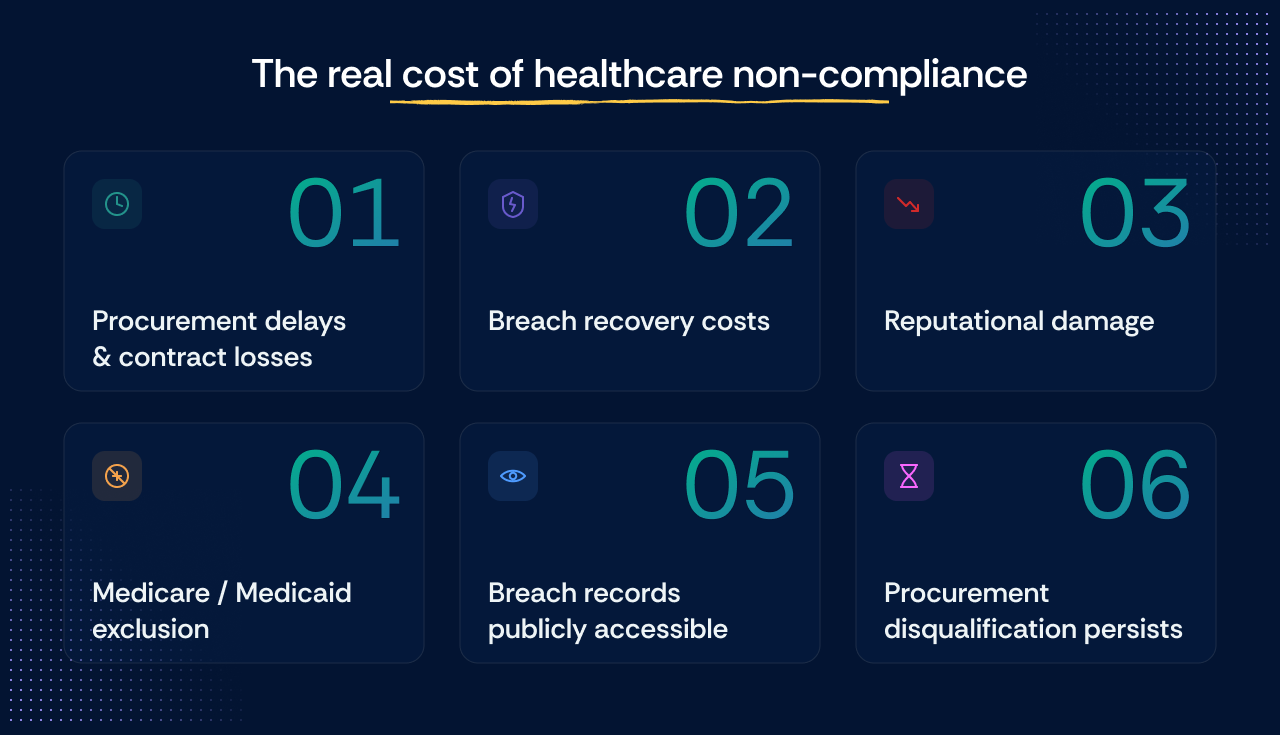
Non-compliance in healthcare is rarely just a regulatory problem. The consequences extend well beyond financial penalties and tend to compound in ways organizations do not fully anticipate until they are managing them.
- Procurement delays and contract losses with hospital and enterprise health system clients
- Breach recovery costs covering notification, forensic investigation, legal counsel, and remediation
- Reputational damage that affects sales cycles for months or years after an incident is resolved
- Exclusion from Medicare and Medicaid participation, which for healthcare-adjacent technology companies can eliminate entire customer segments
- Breach notification records are publicly accessible on the HHS website indefinitely
- Procurement disqualification typically persists well beyond the point of technical remediation, regardless of corrective action taken
How to automate healthcare compliance management
Automation does not create a compliance program. It accelerates one that already has functioning controls, clear ownership, and evidence of discipline.
Most early-stage healthcare startups overbuy compliance tooling before fixing basic operational gaps. Automation amplifies a working program. It does not replace building one.
When evaluating healthcare regulatory compliance software, these capabilities matter most:
- Native integrations with cloud infrastructure, identity providers, and development tools, so evidence flows automatically rather than being entered manually
- Continuous control monitoring that surfaces compliance gaps as they occur, not during audit preparation
- Centralized evidence management with version history and access trails that auditors and procurement teams can navigate without back-and-forth
- Vendor risk workflows covering BAA tracking, subprocessor oversight, and questionnaire management
- Multi-framework support within a unified controls library, reducing duplicated effort across HIPAA, SOC 2, HITRUST, and other applicable standards
- AI governance support for organizations managing tools that process clinical data
Pricing varies by organization size, integration complexity, and the scope of the framework.
Scrut Automation offers an AI platform powered by autonomous agents that operationalize continuous compliance and security. The platform replaces audit chaos with scalable execution, enabling growing businesses to build trust at scale and manage cyber risk effectively.
To explore how Scrut supports healthcare and healthtech organizations specifically, including HIPAA, SOC 2, and vendor risk workflows, visit Scrut’s healthcare solution and get a personalized quote.
HIPAA establishes the foundational privacy and security standards for protecting protected health information. HITECH, enacted in 2009, strengthened HIPAA by making business associates directly liable under federal law, introducing mandatory breach notification requirements, and creating a four-tier civil penalty structure with inflation-adjusted caps. HIPAA sets the rules. HITECH enforces them with significantly greater consequences.
The major regulatory compliance requirements in healthcare include HIPAA’s Privacy, Security, and Breach Notification Rules, the HITECH Act’s enforcement provisions, the False Claims Act, the Anti-Kickback Statute, the Stark Law, state privacy laws such as Washington’s My Health My Data Act, and the 21st Century Cures Act’s information blocking provisions.
Consequences include financial penalties ranging from $145 to over $2 million per violation, breach recovery costs, loss of Medicare and Medicaid participation eligibility, and long-term reputational damage. Breach notifications affecting 500 or more individuals are published publicly on the HHS website and remain accessible indefinitely. Procurement disqualification typically persists well beyond technical remediation.
The OIG’s seven elements of an effective healthcare compliance program (updated in 2023) are Written policies and procedures Compliance leadership and oversight Effective training and education Open lines of communication Well-publicized disciplinary standards Ongoing monitoring and auditing Prompt response to identified issues, including corrective action
The best healthcare regulatory compliance software automates evidence collection, runs continuous control monitoring, manages vendor risk and BAA tracking, and supports multiple frameworks, including HIPAA, SOC 2, and HITRUST, within a unified controls library. Scrut Automation is purpose-built for healthcare and healthtech organizations managing these compliance requirements at scale.





.png)